Age/Sex/Race
52 year old African American male
Chief Complaint
“I am having trouble with distance so I think I need a new glasses prescription.”
Denied having flashes, floaters, pain, itching or burning.
Medical History
Diabetes, hypertension, hepatitis C
His blood sugar that morning was 87.
 Ocular History
Ocular History
Negative
Medications
He didn’t have his medication list with him.
NKDA
Family History
Diabetes and cataracts
Social History
Smokes cigarettes every day, social drinker
Diagnosis and initial plan of action
I thought he might have a refractive error, while some diabetic retinopathy could be evident.
Applicable Testing & Results of Testing
Distance visual acuity (uncorrected):
OD: 20/60
OS: 20/60
Confrontation fields: FTFC OU
Extraocular muscles: Full OU
Pupils: PERRLA, (-) APD
Manifest Refraction:
OD: +3.75 sph, 20/20
OS: +5.50-2.00X165, 20/25
Add +2.25, 20/20 OU
Slit lamp examination:
Lids/lashes – ptosis of upper lid OD
Conjunctiva – racial melanosis OU
Cornea – clear OU
Anterior chamber – no cells and flare
IOP – 12 mm Hg OU
Lens – trace nuclear sclerosis OU
Dilated fundus exam:
C/D: 0.4/0.4 round with distinct borders OU
OD: cotton wool spots nasal to disc
OS: cotton wool spots and flame hemorrhage along superior and inferior arcades
No CSME OU
Assessment and Plan
1) Stage 2-3 hypertensive retinopathy OU vs interferon retinopathy
– Patient mentioned upon further inquiry that he was taking interferon for hepatitis C. He was educated to return to the clinic in 6 months for a dilated fundus examination. When cotton wool spots and flame hemes were observed, hypertensive retinopathy was thought to be the tentative diagnosis. Interferon retinopathy wasn’t initially thought of as a possibility.
2) Cataracts OU: monitor yearly
3) Presbyopia OU: prescribed glasses
4) Involutional ptosis OD
It’s hard to distinguish the cause of retinal changes when a patient has multiple diseases. In order to figure out which disease is the primary reason for the retinal changes, I did some research and found few overall points:
How do you distinguish between hypertensive retinopathy and diabetic retinopathy?
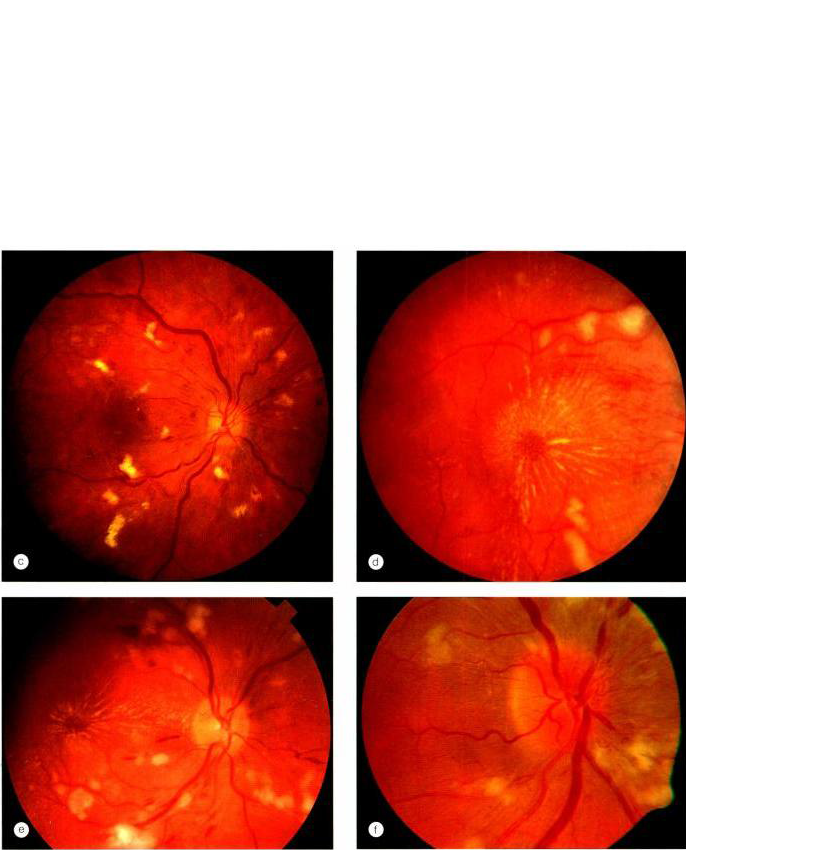
Hypertensive retinopathy: more cotton wool spots are seen than exudates or hemorrhages, while more flame hemorrhages are noticed (3rd picture above, courtesy of Kanski textbook)
Diabetic retinopathy: more hemorrhages are seen, especially dot-blot hemes (2nd picture, courtesy of Kanski textbook)
Interferon associated retinopathy: 1st picture on top
Interferon associated retinopathy has similar signs as hypertensive retinopathy, such as cotton wool spots, retinal hemorrhages and cystoid macular edema. Cotton wool spots are usually around the optic nerve head in interferon associated retinopathy. Usually these signs disappear after stopping treatment. I once heard a speaker say that in some cases, even if these patients have retinal changes, they still have to continue taking interferon for their therapy.
References:
- Shectman, D.L. and Falco, L.A. Hypertension: more than meets the eye. Review of Optometry, September 2007. http://www.revoptom.com/content/d/retina/c/15347/dnnprintmode/true/?skinsrc=%5Bl%5Dskins/ro2009/pageprint&containersrc=%5Bl%5Dcontainers/ro2009/simple
- http://webeye.ophth.uiowa.edu/eyeforum/cases/116-Interferon-retinopathy.htm
- Kanski, Jack J. Clinical Ophthalmology: A Systemic Approach. Philadelphia 2007: pages 484-485

{kind=link}