What do you think of when you hear “strabismus?” Perhaps you think of eye turns like exotropia and esotropia or you may immediately think about surgery…. Well, when I think of strabismus I think “AHHH! What do I do ?!
Okay, well maybe it isn’t a COMPLETE freak-out…. however there is a small part of me that wants to. I mean at this point in my career I feel relatively comfortable working-up and working with a patient who has a CI, AI, OMD, binocular instability, even a person with all of those issues combined, but throw a consecutive XT (this is an XT that occurred post surgery) or a 45-prism diopter ET at me and I clam up!! Luckily at SUNY I had the option to do an externship rotation through the VT/ Pediatrics department. Part of this program gives me the opportunity to experience specialty clinics including strabismus work-ups and vision therapy.
I can honestly admit that the 1st time I had a strabismus patient in my chair I felt completely lost. Having been in this clinic for just over a month now I can tell you that there is so much to learn when it comes to strabismus, but I would like to share with you what I have discovered thus far:
It seems that the best way to approach a strabismus evaluation is to have the basic skeleton of what information you need to make the appropriate diagnosis and treatment plan. Once you have this ‘bare-bones’ template down you can modify (and modify you absolutely will have to!!) based on each individual case.
The Basics of a Strabismus Exam:
1) Case History: Perhaps the most important part of the exam. Try to narrow down the age of onset, any previous surgeries, old doctors records, etc…
For numbers 2-5: Do Distance & Near separately
** It is very important to know the differences between the two**
2) VA: Many cases of strabismus are accompanied by amblyopia; be sure to do whole line VAs as well as single letter VAs. You can even attempt a 2.2x telescope to see if there is any improvement.
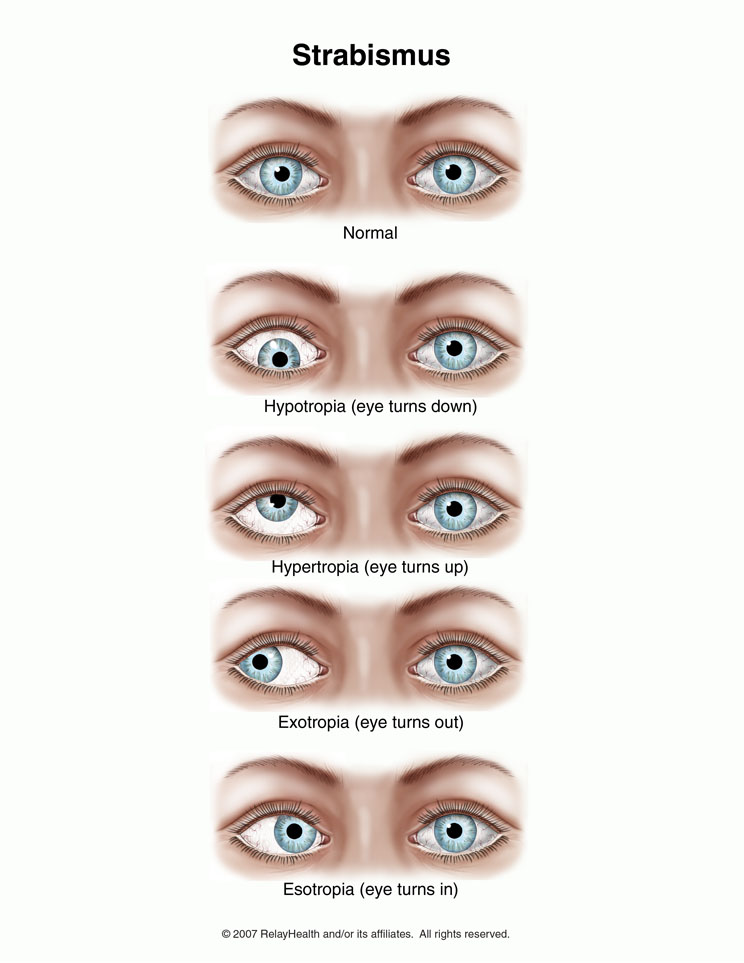
3) Deviation Direction: Is it an XT? ET? Is there a hyper? Hypo? (Make sure to mark down which eye it is!)
4) Deviation Magnitude: Get your prism bars out ladies & gents!! I was given this handy piece of advice so I am sharing it with you: Always neutralize the horizontal component before the vertical component.
5) Constancy of Deviation: Is it intermittent? Alternating? Constant?
6) Comitancy: This may indicate how long the deviation has been present. If it is non-comitant it may warrant further testing.
7) Correspondence: You have to know if your patient has NRC, HARC, NHARC or Paradoxical ARC. How do you do that? Break out those Bagolini lenses, amblyoscope, and after-images. Remember this is a good indication of how much of the binocular system is still intact.
8) Centration: Does your patient use their deviating eye’s fovea or some eccentric point for fixation? Perform visuoscopy or MIT to figure this out . **Don’t forget this is a monocular phenomenon and therefore you must patch the non-deviating eye while assessing the centration!
9) Stereo: Try to get any stereo you can! Play around with the distance to see if you can get any response (i.e. bring stereo book into an ET’s centration point)
* Fun Fact: For RDS you can ask the patient which of the four boxes appears blank. Sometimes patients can get some sort of stereo, but not well enough to make out the shapes. It is important information to know if they see something rather than just nothing at all!
10) Externals: EOMs, NPC, pupils, pursuits, saccades, fixation, free space ranges
11) (Good) Refraction: Getting the prescription right is half the battle.
12) Fusion: Use Worth 4 Dot or a red lens. This should be done at multiple distances seeing if there is flat fusion at any point. You can even do it with the lights on & the lights off to see how deeply imbedded the suppression is.
13) Accommodative testing: Use techniques such as amps, facility or MEM. You don’t have to do these all, but you definitely need to get an idea of their accommodative status.
14) Misc: Keystone, cheiroscopic tracing, VO Star, vectograms, DEM
So there it is… the basics of a strabismus work-up. It may seem like a lot, but all of these variables are necessary to fully understand how a person is using there eyes (and all of their crazy adaptations!) so that you can make a proper diagnosis and further recommendations for treatment.
I’ll leave you with this: the next time (or first time!) you encounter a strab just take a deep breathe, think about what information you need and enjoy the learning experience!
-Mikilyn
